




Sexual life is the most important part of life. Its impact on our life are very deep. It affects our social and personal behaviour. Relationship with our sexual partner is affected by success in sexual life. Job performance,even financial matters also get affected by our sexual life. Healthy sexual life imparts positivity in our sexual relationship, job and other sphere of life. On the other hand unhealthy sexual life worsen our relationship, less efficiency in job and lost peace of mind. Such a disorder of sexual health is Premature Ejaculation, also called early ejaculation. This is very disappointing,embarrassing condition. Female partners in such condition,remains unsatisfied, and male partners even refused to accept it they have any sexual problem due to shame or ego, whatsoever it is.
Facts About Premature Ejaculation
- Premature ejaculation is the second most common sexual problem affecting between 1 in 3 to 1 in 5 men aged 18-59.
- Some men ejaculate as soon as foreplay starts. Others ejaculate during penetration or very soon after.
- One-third to one-quarter of men with premature ejaculation also have problem of erectile dysfunction.
- PE is estimated to affect 30–40% of men at some point in their lives.
- An estimated 30%-70% of American males experience premature ejaculation.
- Polygamous men have a lower incidence of premature ejaculation and higher sexual satisfaction than monogamous men.
- Erectile dysfunction is the leading risk factor for about 36% to 50% of PE.
- Lower frequency of sexual intercourse significantly related to a higher incidence of PE.
- The National Health and Social Life Survey (NHSLS) indicate a prevalence of 30%, which is spread across all adult age groups.
- In almost 75-100% sexual activity, the experience of ejaculation occurring during sexual intercourse within 1 minute after vaginal penetration.
- A large-scale survey conducted by the European Urology Journal found that 20-30% of men between the ages of 18 and 60 report having experienced PE regularly.
- A study published in the British Journal of Urology found that early ejaculation is more common in younger men aged 18-25, with about 25% of them reporting frequent episodes.
- Study by the American Urological Association found that 45% of men with PE reported anxiety and lower self-esteem related to their sexual performance.
- Global Survey of Sexual Attitudes and Behaviors (GSSAB)found that approximately 16% of men globally experience chronic premature ejaculation.
- The Journal of Sexual Medicine in a study found that Lifelong PE results in ejaculation within 30-60 seconds of penetration.
- A study showed that almost 25% of women ended a relationship due to their partners PE.
- PE tends to be under-reported by patients who do not typically seek medical help.
What is Premature Ejaculation?
Premature ejaculation is defined as a condition where a man ejaculates within one minute of vaginal penetration and is unable to control it, causing distress to either the man or his partner. The average intravaginal ejaculatory latency time (IELT) for men with PE is under 1-2 minutes. Most men without PE ejaculate within 5-6 minutes of penetration. The Intravaginal Ejaculatory Latency Time (IELT) is the average time between vaginal penetration and ejaculation estimated by the patient. Also if a person makes less than 60 penile strokes in one minute continuous with stopping,he may be suffering from premature ejaculation. PE can be a frustrating experience for both partners and can make sex less enjoyable. International Society of Sexual Medicine (ISSM) defined PE as a male sexual dysfunction characterized by:
- Ejaculation which always or nearly always occurs prior to or within about 1 minute of vaginal penetration;
- Inability to delay ejaculation on all or nearly all vaginal penetrations;
- Negative personal consequences, such as distress, bother, frustration and/or the avoidance of sexual encounters.
If PE causes you (or your loved one) to worry or to feel stressed, then you should ask your Sexologist for help. Remember that you are not alone, and your Sexologist knows what to do. Together, you can find the underlying cause and find treatment.
Types of Premature Ejaculation
There are two main types of Premature Ejaculation: 1.Lifelong PE (Primary) 2.Acquired PE (Secondary)
- Lifelong Premature Ejaculation:-The person has been experiencing premature ejaculation since he became sexually active.Usually it is seen that premature ejaculation starts from the beginning of his sexual activity probably the first sexual intercourse or on masturbation as well.
- Acquired Premature Ejaculation:- Acquired premature ejaculation means that the condition began in an individual who previously have satisfactory level of ejaculatory control and had successful sexual relationships and only now has developed premature ejaculation in the recent past.
PE can range from mild to severe, depending on how soon it occurs after penetration:
- Mild: Occurs within 30 seconds to 1 minute of penetration.
- Moderate: Occurs within 15–30 seconds of penetration.
- Severe: Occurs before sexual activity, at the start of sexual activity, or within 15 seconds of penetration.

Four Subtype of Premature Ejaculation
| Lifelong PE | Acquired PE | Variable PE | Subjective PE |
| Hypertonic State | Hypotonic State | Normotonic State | Normotonic State |
| Type B | Type A | ——- | ——– |
| Erectio praecox | No Erectio praecox | No Erectio praecox | No Erectio praecox |
| Detumescentia praecox | No Detumescentia praecox | No Detumescentia praecox | No Detumescentia praecox |
| IELT<1 | IELT= 1<3 | Variable IELT | Normal IELT |
| Neurobiological and Genetic | Medical and/or Psychological | Normal variation | Psychological |
| Consistent | History of normal ejaculation earlier | Inconsistent | Subjective perception of PE despite normal ejaculation |
Lifelong PE

Acquired PE
Variable PE

Subjective PE
Sign & Symptom Of Premature Ejaculation
In most cases of premature ejaculation patient does not reveals exact situation. PE may be associated with other sexual dysfunctions such as erectile dysfunction, decreased libido etc. These signs are common in all patient of PE:-
- A short ejaculatory latency;
- A lack of control over ejaculation;
- A lack of sexual satisfaction.
The four main interweaving sets of symptoms are:
- Short IELT, with Control;
- Short IELT, No Control;
- Normal IELT, No Control;
- Normal IELT, with Control.
Physiology Of Premature Ejaculation
Ejaculation is the sudden, pleasurable release of semen through the penis. It is controlled by your brain i.e.your central nervous system. When you are sexually stimulated, signals are sent up through your spinal cord to your brain. When you reach a certain level of excitement, your brain tells your reproductive organs to “go!” This causes semen to be ejected through the penis called ejaculation. Ejaculation has two phases: emission and expulsion.
- Phase 1:Emission:- Emission is when sperm moves from the testicles to the prostate. There it mixes with seminal fluid to make semen. The vasa deferentia are the tubes that help move the sperm from the testicles through to the prostate to the base of the penis. Parasympathetic is responsible for epithelial secretion, while the sympathetic nervous system is responsible for tonal control and contractions of smooth muscle in the seminal trait. Activated by genital or cerebral erotic stimulation. In emission phase sequential contractions of accessory sexual glands occurs. Emission is dependent on contractions of the smooth muscles of the prostate, seminal vesicles, and vas deferens, and its initiation can be voluntarily controlled. Once the semen reaches the posterior urethra, ejaculation becomes inevitable. The male organs involved in the emission process are Epididymis,Vas deferens,Seminal Vesicles,Prostate and Bulbourethral i.e. Cowper glands.
- Phase 2:Expulsion:- Expulsion is a spinal cord reflex that occurs as the ejaculatory process reaches a “point of no return.”Expulsion is when the muscles at the base of the penis contract. This forces semen out of the penis. Often, ejaculation and orgasm (climax) happen at the same time. Some men climax without ejaculating. In most cases, erections go away after this phase. It is controlled by somatic and sympathetic nervous system. Activated by sensation resulting from distension of posterior urethra. In expulsion phase rhythmic contractions of bulbocavernosus,ischiocavernosus and levator ani muscles take place.These contractions occur rhythmically at 0.8-s intervals. These rhythmic contractions are extremely pleasurable and are part of the sensation of orgasm. A young healthy individual has 10 to 15 contractions per ejaculation. The organs involved in expulsion are smooth muscles of Bladder neck,Stratified epithelium of Urethra and Pelvipereneal striated muscles.
Pathophysiology of lifelong PE is mediated by a very complex interplay of central and peripheral serotonergic, dopaminergic, oxytocinergic, endocrinological, genetic and also epigenetic factors. Characterized by a diminished central 5-HT neurotransmission and/or a hyperfunction of 5-HT1A receptors and a hypofunction of 5-HT2C receptors causing a disturbed serotonergic modulation of the IELT. Therefore, it would have to include serotonergic and other neurotransmitter and endocrinological processes—e.g., increased oxytocinergic, and/or increased dopaminergic neurotransmission, decreased Prolactinergic functioning and increased activity of gonadotrophic factors. Also involved is the peripheral nervous system, e.g., the sympathetic and parasympathetic nervous system.Physiology of PE involve disturbance in any of the following mechanisms:
- Penile Hypersensitivity;
- Hyperexcitable Ejaculatory Reflex;
- Hyperarousability;
- Genetic predisposition;
- 5-hydroxytryptamine (5-HT)-receptor dysfunction.
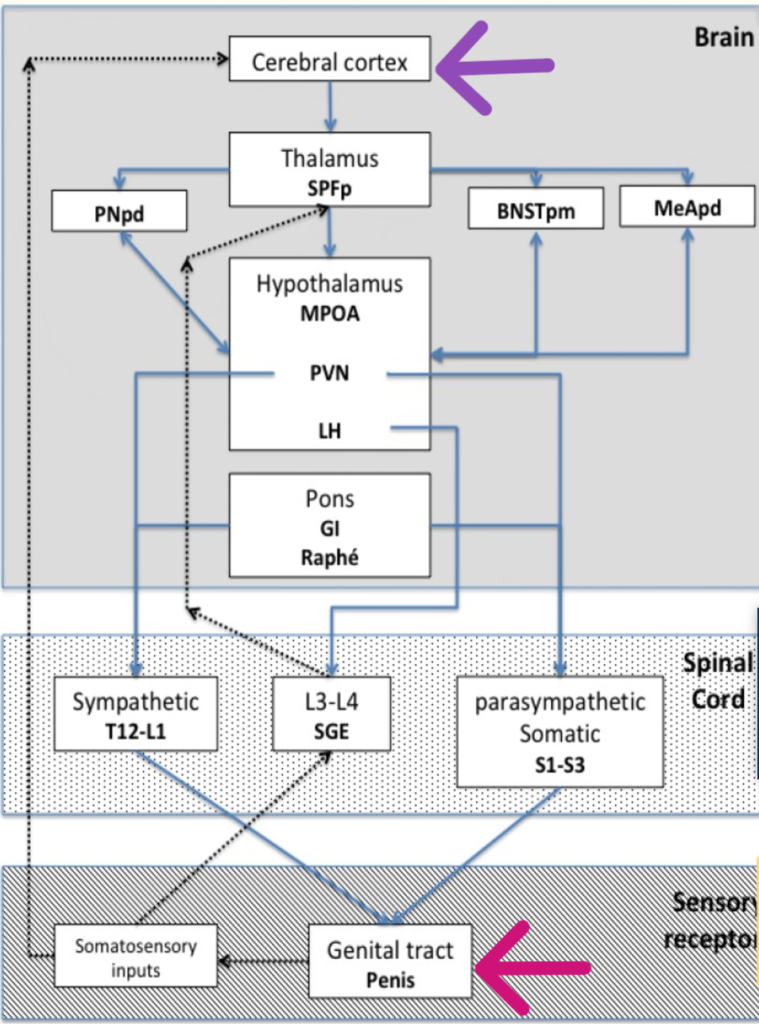
Process of ejaculation is controlled by some cerebral areas. The cerebral areas that actively participate in ejaculation are the posteromedial division of the bed nucleus of the striaterminal (BNST pm), the posterodorsal area of the amygdala (MeApd), the posterodorsal preoptic nucleus (PNpd)and the parvicellular part of the subparafascicular thalamus (SPFp). One of the most important excitatory paths includes neurons in the preoptic medial area (MPOA)that project in the paraventricular hypothalamus (PVN). The inhibitory centres originate from neurons in the gigantocellular nuclei (Gi) and ventral raphe in the ventral medulla. Spinal part include Preganglionic sympathetic neurons located in the intermediolateral cell column and the dorsal grey column (T12- L2) innervate the urogenital area. Preganglionic parasympathetic that innervate the urogenital area are found in intermediolateral cell column between S2-S4. Somatic neurons responsible for motor innervation of pelvipereneal and urethral sphincter are found on the Onuf nucleus on the ventral horn of S2-S4. A component to the generation of ejaculation was identified on the lumbar region of L3-L4.These spinothalamic neurons segments, also known as spinothalamic ejaculation generators, coordinate the autonomous and somatic (pudendal) processes, in order to initiate ejaculation.Activation of the autonomous nervous system and the somatic nervous system is essential for ejaculation [as is the role of non-adrenergic non-cholinergic (NANC) in modulating the activity of accessory glands].
Many Neurotransmitters take part in the process of ejaculation, which are at peripheral level are Norepinephrine, Acetylcholine, Nitric oxide, Oxytocin, Purines, Serotonin and at medullar level are GABA, Oxytocin, P substance and at central level are Serotonin, Dopamine, Opioids, Oxytocin.
Causes of Premature Ejaculation
The exact cause of PE is not known, but there are many reasons why a man may have PE. PE can be caused by a number of factors, including: Biological factors, such as inflammation of the prostate gland or a spinal cord problem. Chemical factors, such as abnormal hormone levels. Emotional factors, such as anxiety, stress, or relationship problems. Genetic factors related to the molecules that signal between nerves. Serotonin is a natural substance in your body made by nerves. It helps to control the way the brain manages mood, emotion, sleep and sexual desire. High amounts of serotonin in the brain increase the time to ejaculation. Low amounts can shorten the time to ejaculation, and lead to PE. Below are some more specific causes.
Psychogenic Factors
Psychological, or mental health, issues can be involved with PE and may include:
- Depression
- Anxiety
- Stress
- Guilt
- Unrealistic expectations about sex.
- High Arousability.
- Early sexual experience: doing sexual activities in hurry in fear of being caught.
- Lack of awareness of techniques effective in ejaculatory control.
- Lack of confidence.
- Frequency of sexual activity: less frequent sexual behavior.
- History of sexual repression (blocked sexual feelings).
- Relationship problems.
- Deep seated hatredness, personality disorders.
Biogenic Factors
- Endocrinological causes:- Diabetes, Hyperthyroidism.
- Penile sensitivity:- Hypersensitivity i.e. raised sensation of penis.
- Urological conditions:- Prostatitis.
- Chronic renal insufficiency.
- Neurological diseases:- Multiple Sclerosis, peripheral neuropathies.
- Sexual disorders:- Erectile Dysfunction: Compensatory effort to achieve ejaculation before the loss of the erection and Loss of Libido.
- Varicocele.
- Low vitamin B12 levels.
- Low seminal magnesium levels.
- Increased serum leptin levels.
- Drug induced:- Amphetamine, cocaine, and dopaminergic drugs.
Genetic Factors
- Polymorphisms of the 5-HTTLPR gene:- Polymorphisms of the serotonin transporter promoter region gene, of chromosome 17, which encodes the serotonin-transporter-linked promoter region (5-HTTLPR) have been investigated in many studies exploring the genetic basis of PE. The 5-HTTLPR gene has two variant alleles: a short (S) and a long (L) allele. 5-HTTLPR is associated with lifelong PE and L alleles might protect the male against lifelong PE.
- 5-hydroxytryptamine receptor dysfunction:- 5-HT2C receptor hyposensitivity and/or 5-HT1A receptor hypersensitivity.
Diagnosis Of Premature Ejaculation
An accurate clinical history is the best diagnostic method, and in the majority of the cases it is enough to differentiate between primary and acquired premature ejaculation. Clinical history plays an important part in the diagnosis of PE since it is by definition a self-reported diagnosis. However, clinical assessment can be challenging owing to the nature of the problem. Patients may be embarrassed and shy when relating details of their sexual experiences and exact details are not forthcoming. It may then be useful to involve the partner in the consultation. To elicit a diagnosis of PE, the three main components of PE (timing, control and satisfaction) should be specifically addressed. Once a diagnosis of PE is established, other related things that should be explored are:
- The nature of the PE (lifelong or acquired);
- The presence or absence of any associated erectile dysfunction (ED);
- The impact of the PE on the relationship with his partner;
- The impact of the PE on quality of life;
- Previous Treatment (including over the counter medication) and response to that treatment.
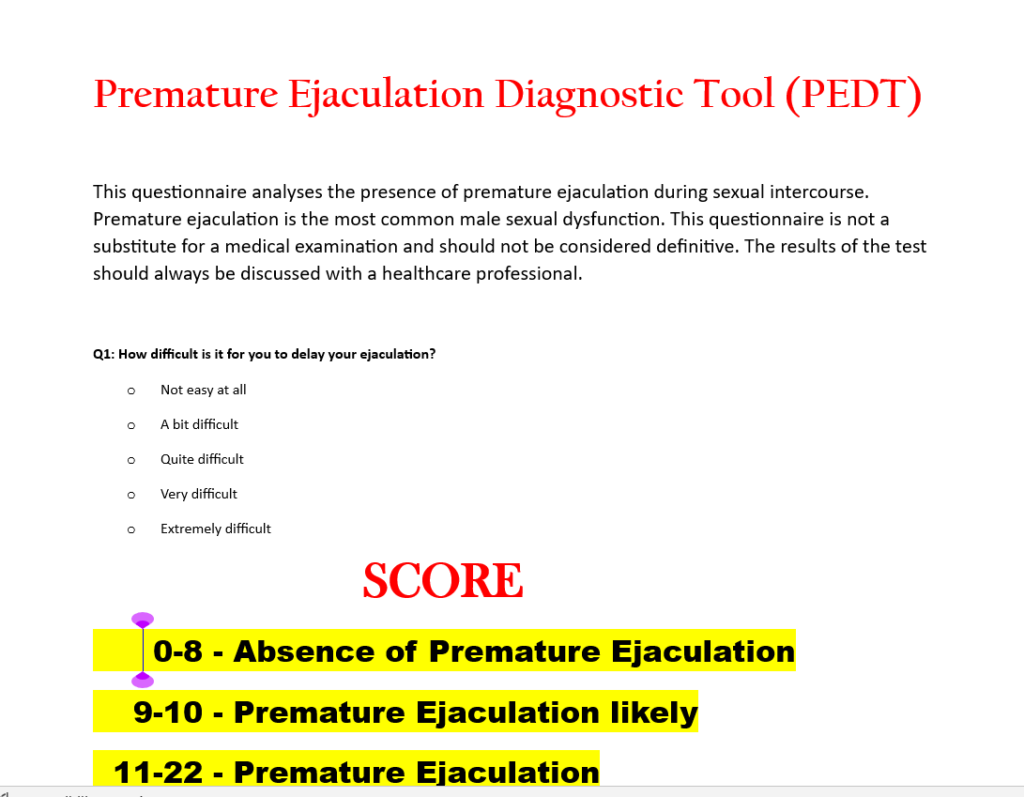
Questionnaires
For this purpose Questionnaires such as the Index of Premature Ejaculation i.e. IPE, the Premature Ejaculation Diagnostic Tool i.e. PEDT, Premature Ejaculation Profile i.e. PEP, Arabic Index of Premature Ejaculation i.e. AIPE, Chinese Index of Premature Ejaculation i.e. CIPE can be used. Premature ejaculation diagnostic tool (PEDT) is consisted of five questions. This is a questionnaire to help identify men who may have a problem with ejaculating too soon during sexual activity. Even if you do not have difficulties, please answer all the questions.
A score of < 8 equals No PE, A score of 9 or 10 means Probable PE, and A score of > 11 indicates PE.
Physical Examination and Tests
Examination:- Physical examination is usually normal in patients with Primary PE. Patients with Secondary PE, may have an altered physical exam that suggest presence of anatomical anomalies and disorders. Examination of the patient involves a general examination as well as a more focused examination of the genitalia, outlining the scrotal contents and the penis in detail. A digital rectal examination to palpate the prostate gland is also recommended. Clinical examination can identify anatomical anomalies, disorders and risk factors that may favor PE.
- Shortness of the frenulum, pathology of the Prepuce (Phimosis) or Glans (Balanitis);
- Other anatomical anomalies of the urogenital system;
- Examination of the perineum and Prostate (Prostatitis);
- Search for signs of Dysthyroidism.
Laboratory Tests:- Laboratory and other physiological tests are rarely indicated. History and examination are sufficient to reach a diagnosis. Still it is advised to perform, blood count, lipid profile, glycosylated haemoglobin, urinalysis, testosterone (free and total), prolactin and thyroid stimulating hormone (TSH).
Treatment Of Premature Ejaculation
Nowadays the treatment PE is not curative, but is effective in increasing the Intravaginal Ejaculatory Latency Time, improving the couple’s sexual satisfaction. You and your Sexologist can work together to decide the best choice for you. Many people try more than one treatment at the same time. Psychological therapy, Behavioral therapy and drugs are the main treatments for PE. The first oral medication used for the treatment of PE were monoamine oxidase i.e.MAO inhibitors,such as Isocarboxazid, Phenelzine; and Alpha-1 adrenergic blocking agent,such as Phenoxybenzamine, alfuzosin, terazosin. However, the side effects associated with these drugs limited their use. These agents are not used for PE anymore.
Psychological Therapy
Psychological therapy is a way to work through the feelings and emotions that may lead to problems with sexual relationships. The goal of this type of therapy is to learn the source of problems and find solutions that may help PE. You might want to involve your sexual partner in discussions about how to manage premature ejaculation because the issue may affect their sexual satisfaction, and there may be things they can do to help. It can also help couples learn to grow closer. Psychological therapy can help you become less nervous about sexual performance. It can also give you greater sexual confidence and understanding to help your partner’s satisfaction. Psychotherapy involves educating both the male patient and the female partner. This can happen in the context of relationship counselling as well as psychosexual therapy. Meditation is also included in this therapy.This type of therapy can be used as the only treatment, or it may be used along with medical or behavioral therapy.
Behavioral Therapy
Behavioral therapy uses some techniques and exercises to achieve delay in ejaculation. The goal is to help you train your body for long time in sex. Some techniques are the squeeze method and the stop-start method and Kegel exercises. Sexual therapy focuses on perception and feelings with the goal of improving communication between partners, increasing sexual skills, self-confidence and reduce anxiety during sexual intercourse. It is believed that behavioural therapies result in increased IELT.
- Stop-Start Method:- In this method, you and your partner stimulates your penis until just before ejaculation. When you are about to ejaculate, you and your partner stops until the urge to ejaculate lets up. As you regain control, you and your partner start stimulating your penis again. This process is repeated three times. You ejaculate on the fourth time. You repeat this method three times a week until you have gained more control.


- Squeeze Method:- With this method, you and your partner stimulates your penis until you are close to ejaculation. When you are close, you or your partner firmly squeezes your penis just below the glans so your erection partly goes away. The goal is for you to become aware of the sensations leading to climax. The squeeze method may help you better control and delay ejaculation on your own.
- Pre-coitus masturbation:- Masturbation before intercourse can delay the ejaculation.
- Kegel Exercise:- Pelvic floor muscles exercise will help to gain control over ejaculation. Kegel will increase your capacity to hold the semen.
- Climax Control Condoms:-Trojan Extended Pleasure condoms come with Climax Control Lubricant to help keep you going while you’re going at it. The clear lube has a special active ingredient to help prevent premature ejaculation and provide greater staying power.These condoms have a special lubricant that is formulated with a numbing substance, typically benzocaine. Your most sensitive nerve endings are found at the tip of your penis, and this lube lessens the sensation in that part. Durex Extended Pleasure,Trojan Extended Pleasure, are helpful in PE.
- Sensory Abstraction and Thought Redirection:- Divert your attention from sexual act for 2-3 sec when you are about to ejaculate.
- Disease-targeted treatment:-If premature ejaculation is related to erectile dysfunction, treating the erection problem might solve the ejaculation problem.In these patients, depending on aetiology, it is recommended physical activity, weight loss, abstaining from alcohol, treatment of hyperthyroidism and hypogonadism, strict glycaemic control in diabetic patients and antibiotics in patients with chronic bacterial prostatitis.

Medical Therapy
No drugs have been approved in the United States to treat PE except Dapoxetine. Still, there are a number of drugs, numbing creams and numbing sprays that slow ejaculation in men with PE and are used off label.At the present time, only one drug, dapoxetine is licensed for the treatment of PE. However, the other drugs described below can also be used, as long as the patient is fully aware that they are not licensed for the treatment of PE. Drugs for PE can be taken each day or only before sex. Your Sexologist will advise when you should take a drug based on your activity level. PE can return if you stop taking these drugs. Most men with PE need to take these drugs on an ongoing basis. So Herbal treatment is advised for long term solution and no side effects.
- Dapoxetine:-Serotonin is the most important neurotransmitter in ejaculatory control. Dapoxetine is an Serotonin Selective Reuptake Inhibitor (SSRI) with fast onset of action. Available in tablet form ‘Priligy’ of 30 mg and 60 mg. It is contraindicated in cases of moderate to severe hepatic disease, heart failure, ischemic cardiac disease and carriers of pacemakers.
- Desensitisers:- Topical creams and spray are used to achieve numbness in the penis such as EMLA,SS Cream,TEMPE i.e.PSD502.The combination of lidocaine and prilocaine topical anaesthetics are the used for the treatment of PE. A creme with 5%lidocaine-prilocaine is effective in increasing mean IELT 6 to 8 minutes. Cutaneous spray solution of lidocaine (150 mg/mL) and prilocaine (50 mg/mL) is used to treat PE. Spray solution applied to the gland is rapidly absorbed in non-keratinized epithelium and has effect 5 minutes right after application. It is odourless, doesn´t require the use of a condom. Side effects are hypoesthesia, loss of erection, genital erythema and local burn. SS–cream (Severance Secret cream) is made up of extracts from 9 natural products for treating premature ejaculation (PE).


- Selective serotonin reuptake inhibitors:- SSRIs can be used to treat PE.Sertraline 50–200 mg, fluoxetine 20–40 mg and citalopram 20–40 mg and Duloxetine and Escitalopram Adverse effects include fatigue, yawning, mild nausea, loose stools, or perspiration.
- Tricyclic antidepressants:- The most used drug for this group is clomipramine in the dosages of 10 to 50mg.By inhibiting the reuptake of catecholamines, it increases the adrenergic effects.
- Central acting opioid analgesic:- Tramadol can increase IELT.Mechanism of action may be due to modulation of the nervous central system, reuptake of serotonin and norepinephrine.
- Surgery:- The main surgical approaches for the management of PE include: (i) dorsal nerve neurectomy (DNN),(ii) (CT)-guided cryoablation of dorsal nerve ablation and neuromodulation of the dorsal nerve (NMDN). Despite the surgical interventions are commonly used in Asia, the guidelines do not recommend any type of intervention for PE.
- Future treatment:-1.Resiniferatoxin may be future treatment options for PE. 2. 9-HC-6-one:- 9-hydroxycanthin-6-one, a β-carboline alkaloid isolated from Eurycoma longifolia.
Herbal Therapy
Herbal treatment for PE is the best treatment in my opinion because of no side effects and long lasting. Many herbs are used to treat PE some of them are listed below:
- Akarkara
- Irani Akarkara
- Salam Mishri
- Shilajit
- Brahmi
- Amla
- Gokshura
- Keeda jadi (Cordyceps sinensis)
- Ashwagandha


FAQ About PE
What is Premature Ejaculation?
It is the inability of person to control the ejaculation in sexual intercourse so that it occurs early than he wants.
What causes Premature Ejaculation?
Sometimes it is due to psychogenic factors, and in others may be due to biogenic factors.
Is Premature Ejaculation permanent?
No, it can be managed by some techniques in sex and medicines.
What is the normal time of ejaculation?
There is not a defining criteria for normal ejaculation time. According to medical point of view if a person is capable of doing continuous intercourse without ejaculating more than one minute is normal.
Do women ejaculate?
Some women do report release of fluid at the time of orgasm, but this is rare.
What is Nightfall?
Night fall is the involuntary ejaculation of semen while in sleep.
What is Dhat Syndrome?
When a man exerts pressure during defecation, some drops of urethral fluid comes out through penis is called Dhaat. This is not semen, but fluid from seminal vesicles.
Can I get my female partner pregnant even i am suffering from PE?
Yes, you can get your female partner pregnant even if you are suffering from Premature Ejaculation provided sperm count and motility is normal.
Can premature ejaculation be cured?
Yes, premature ejaculation is treatable.
Can premature ejaculation cause infertility?
No. Premature ejaculation doesn’t cause infertility.
What are the medicines for premature ejaculation?
Herbal medicines are the best medicine to treat the PE.
Can a man have premature ejaculation without erectile dysfunction?
Yes, a person can have premature ejaculation even if he is not suffering from erectile dysfunction.
What is the fastest way to cure PE?
You and your Sexologist can work together to decide the best choice for you. Many people try more than one treatment at the same time.
Which drinks delay ejaculation?
Water. Water is essential for health and hydration, Aloe Vera, Pomegranate Juice, Milk, Watermelon Juice, Banana Shake.
Which food delay ejaculation?
Dark chocolate and Bananas.